Approximately 4,500 patients a year receive radiation treatment at The University of Kansas Cancer Center, one of 56 National Cancer Institute-designated comprehensive cancer centers in the United States. In June 2023, the center became one of the first radiotherapy providers to go clinical with the Eclipse treatment planning system v18.0 on its fleet of ten Varian treatment delivery systems. Calling the upgrade from Eclipse v15.6 to v18.0 “seamless,” Director of Treatment Planning, Dr. Kenny Guida, DMP, DABR, shares his perspective on -- and enthusiasm for -- the enhanced efficiency and accuracy that v18.0 brings to their busy, high-volume environment.
Top image: Dr. Harold Li, PhD, FAAPM, Professor, Vice Chair/Chief of Physics in the Department of Radiation Oncology (left) with Dr. Kenny Guida, Assistant Professor and Director of Treatment Planning in the Department of Radiation Oncology at The University of Kansas Cancer Center.
What feature or improvement in Eclipse v18.0 has had the biggest positive impact at your clinic?
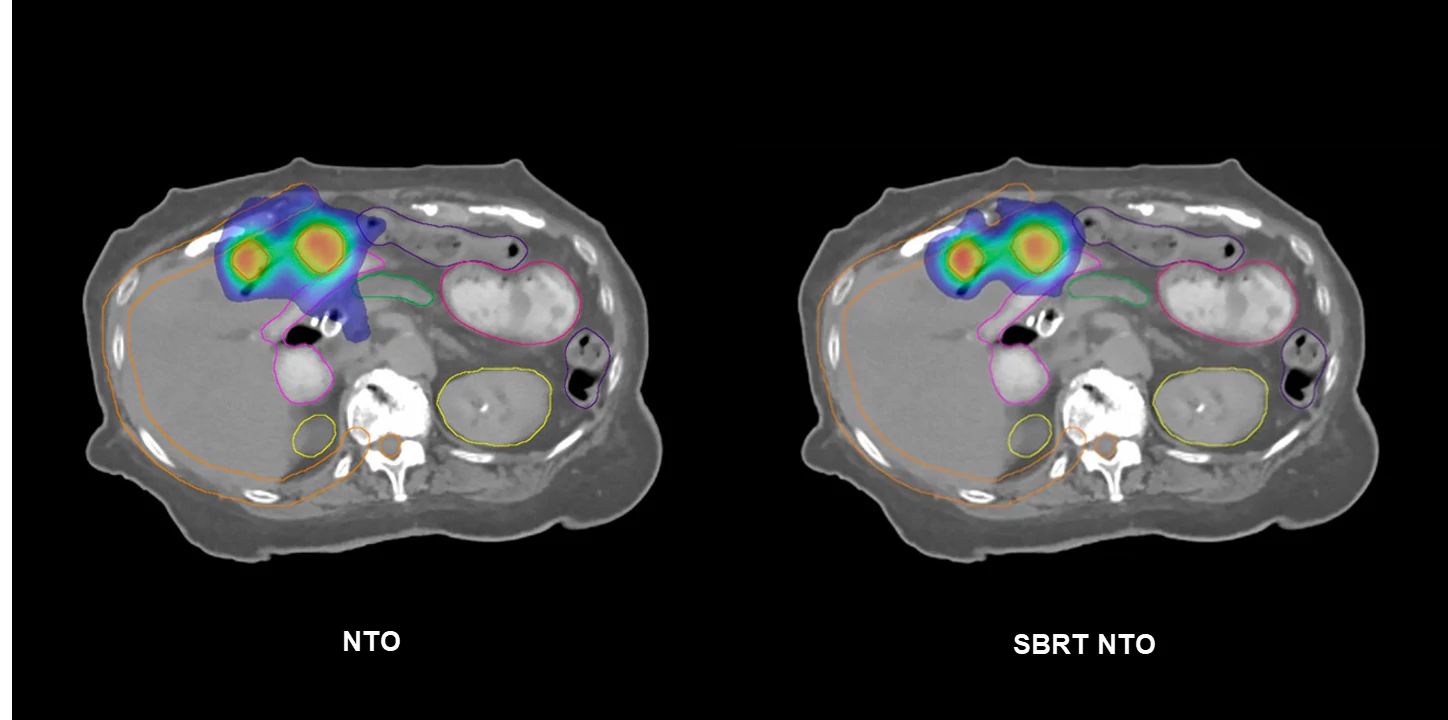
As a physicist who loves treatment planning, I would say the improvements in the Photon Optimizer (PO) have been a game changer. The Fourier Transform Dose Calculation (FTDC) advancement is one of the best things that’s happened in terms of efficiency and accuracy in the optimization process. It was eye-opening how close FTDC is to Monte Carlo and Acuros XB1 ; much closer than MRDC (multiresolution dose calculation) ever was. In addition, GPU improvements dramatically speed up optimization. PO in v18.0 also provides the ability to use SBRT NTO (Normal Tissue Objective) for the first time, which is another tool that our team has come to utilize for a variety of stereotactic cases.
What impacts has Enhanced Leaf Modeling (ELM) had in your clinic and what might it do for other clinics?
ELM is a step forward in more accurately modeling the MLC leaf tip end and drive screw and beam divergence. We’re seeing closer agreement between predicted and measured dose distributions, presumably due to improved MLC modeling.
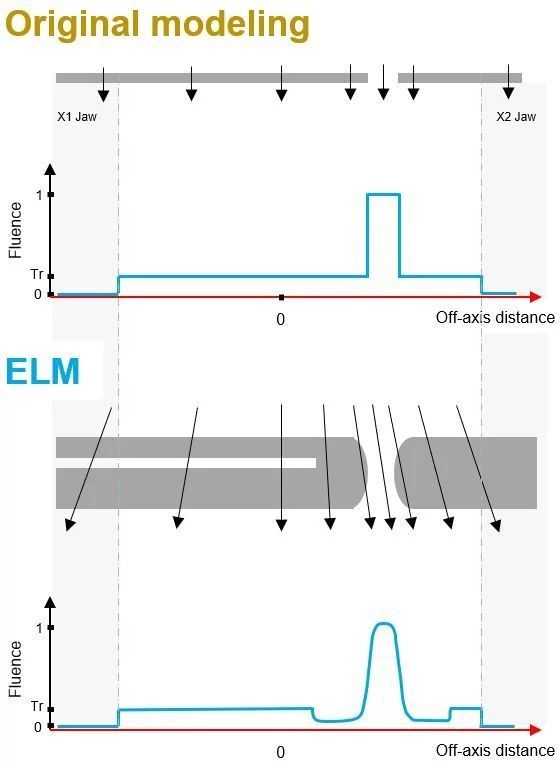
Before we went clinical with Eclipse v18.0, our physics team performed ELM measurements for our 10 linear accelerators using the DICOM files and guidance provided by the Varian team. [Note: Centers can upgrade to Eclipse v18.0 and use their previous DLG measurements to configure ELM or continue with previous beam models until ready to use ELM.]
We recreated many of the tests reported in the research paper by Ann Van Esch2 et al. Our testing showcased, among other positive observations, how much better ELM was in modeling the leaf tip and off-axis dose distributions, which are both critical in radiation therapy today with the increased use of small fields in SRS and SBRT.
We recently commissioned a Varian Edge system equipped with HyperArc, so understanding the impact of ELM on single-isocenter multi-target treatments was important to our physics team. Recent measurements using EBT4 indicated a difference within 2 percent between measured and v18.0 dose predictions for Zebra fields, even at a 12-centimeter off-axis position. When applied to HyperArc plans, which involve delivering precise high dose beamlets across the entire field, these measurements align much more closely with the predictions in Eclipse, and thus should make a big impact on the accuracy of patient treatments.
I have rerun QA analyses on several plans with both our v15.6 and v18.0 algorithms and compared them to our measured results. Especially for smaller fields and those that are highly modulated, we are seeing improvements in IMRT QA pass rates. Even for the Static Wallpaper Test, a simple 16cm x 15cm field with static 4-cm openings, it was eye-opening to see the impact of ELM and the improvements in dose modeling on quality assurance measurements. Our gamma passing rates, using 2%/2mm for MapCheck 3 and EPID, improved from 92.7% and 89.5% to 97.3% and 97.2%, respectively.
What about GPU? How have the improvements been received at KU?
Our dosimetrists tell us that GPU is their favorite feature of Eclipse v18.0. With the demand for high-quality plans in a high-volume workplace, GPU assistance in VMAT planning has been a vital asset for our dosimetry team.
VMAT. We reran 40 VMAT patients, including a variety of disease sites, as well as HyperArc, with PO in both v15.6 and v.18.0. When using PO v18.0 with FTDC without GPU, we saw an average time savings of 2.5 minutes (30%) over PO v15.6. Turning on GPU saved six minutes on average, a 75% reduction in plan optimization. Using GPU in PO v18.0 saved more than 60% on plan optimization time as compared to PO v18.0 without GPU.
SBRT. In a similar study, I ran 50 SBRT lung cases with PO v15.6 and PO v18.0, with and without GPU. With convergence mode enabled, PO v18.0 with GPU averages four minutes to optimize a plan from MR Level 1 through 4. Without GPU, the average time to optimize is ten minutes. By contrast, with PO v15.6, these same optimizations ran 16 minutes, on average.
MCO and plan libraries. With Eclipse v15.6, we gained MCO. I loved MCO immediately but some of our dosimetrists were skeptical about the time involved in creating treatment plans with it. Now with v18.0, we have GPU to speed up the process and our dosimetrists use MCO a lot more.
Adaptive planning. GPUs can significantly open pathways for offline adaptive planning. We’re seeing more patient plans being adapted and having GPU and a robust knowledge-based planning program has enhanced our photon planning to ensure that patients have a high-quality VMAT plan.
What is your experience with the new MCO Isodose line dragging?
With MCO isodose line dragging, planners can interactively see, in real time, the effect of tradeoffs in a plan. For example, if one of our physicians doesn’t want to see 54 Gy on the brainstem, the planner can show the physician alternative possibilities by dragging the 54 Gy isodose line away from the brainstem using a simple touch on the screen. Isodose line dragging gives us another tool to tailor each patient’s plan specifically to the physician intent.
Has SBRT NTO been a useful tool in minimizing manual work such as creating optimization rings in your plans?
SBRT NTO has reduced my reliance on rings for SBRT planning. I was accustomed to using 2-3 rings, depending on the plan, to bottle up high and intermediate dose to improve conformity. Now, I turn my SBRT NTO on and bump up the priority to match my target structures, and I observe improved conformity.
SBRT NTO has a place in the clinic for many body sites, especially as clinics are treating more oligometastatic disease. For cases where a planner is treating multiple targets in the lungs or liver, SBRT NTO aims to drive conformity and reduce dose bridging without having to add additional avoidance structures.
What was your overall experience of the upgrade process to v18.0?
While any upgrade can be stressful, we had the full support of our team at The University of Kansas Cancer Center, including our Department Chair, Dr. Ronald Chen, and Chief of Physics, Dr. Harold Li. We jumped from v15.6 to v18.0, so we were provided with new tools and enhancements from v16.1, such as clinical goals, coupled with the new features in v18.0. Being part of the launch program gave us time to explore the new features—MCO isodose line dragging, FTDC, and especially Enhanced Leaf Modeling—so that we were ready to implement these updates right after the upgrade. There was no machine downtime and no issues impacting patient treatments whatsoever. Our experience with Eclipse v18.0 has been overwhelmingly positive.
- Laakkonen, Linda, et al. “Technical note: TERMA scaling as an effective heterogeneity correction model for convolution-based external-beam photon dose calculations.” Med Phys, 2023, 1-8. DOI: 10.1002/mp.16268
- Van Esch, Ann, et al. “Testing of an enhanced leaf model for improved dose calculation in a commercial treatment planning system.” Med Phys, 2022, 1-12. DOI:10.1002/mp.16019
The information captured herein represents the genuine experience of the attributed individuals and may not necessarily represent the views of Varian or the above-referenced institution. Individuals were not compensated for their participation.